The Courage of a Thirteen-Year-Old Girl Who Refused to Let Scoliosis Define Her Life
The Girl Who Loved School
At thirteen, Chandana was like every other girl in her class. She loved going to school, laughed with her friends during lunch breaks, and dreamed of becoming a teacher one day. Her school uniform was always neat, her homework was always complete, and she never needed to be reminded to get ready for school.
Then, one morning, she refused to go.
“I don’t want to study anymore,” she told her parents quietly.
Her mother looked at her in disbelief.
“What do you mean? You’ve always loved school.”
“I’ve just lost interest.”
Her father thought it was a passing phase.
“Everyone gets tired of school sometimes. You’ll be fine.”
But Chandana remained firm. She refused to wear her uniform, pack her books, or even step outside the house. Her parents tried everything—reasoning with her, encouraging her, even scolding her. Nothing worked.
The Secret She Had Been Carrying
After hours of gentle persuasion, Chandana finally broke down.
“I can’t bear it anymore,” she sobbed.
“The boys call me names. They laugh when I walk.
Even children on the street stare at me and whisper about my bent back.
I don’t want anyone to see me.”
Her mother was stunned. She suddenly remembered a conversation nearly a year earlier.
“Amma, does my back look different?”
At the time, she had glanced briefly and reassured her daughter.
“It’s probably because of your heavy school bag. Don’t worry.”
Believing her mother, Chandana ignored it. But the curve slowly became worse. At first only she noticed it. Later her clothes fitted differently. Soon everyone noticed. The whispers became laughter. The laughter became mockery. Classmates mimicked the way she walked. Children on the street made cruel comments. Each insult gradually weakened her confidence. She stopped looking into mirrors. She stopped making eye contact with people. Finally, she stopped going to school.
A Diagnosis That Changed Everything
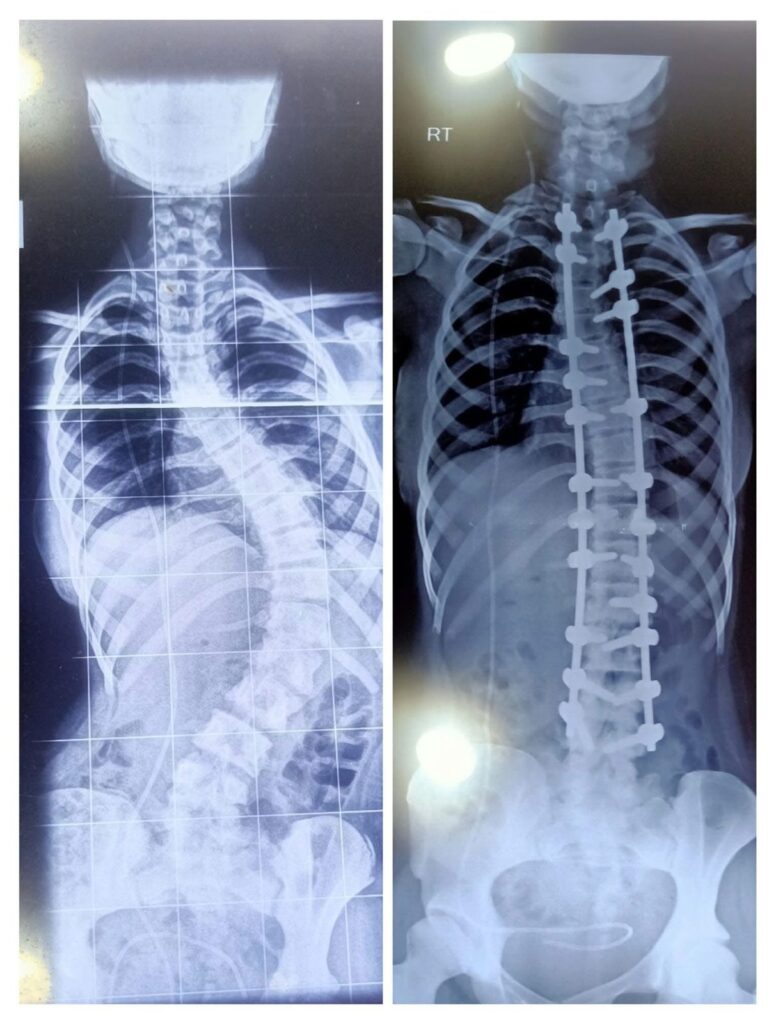
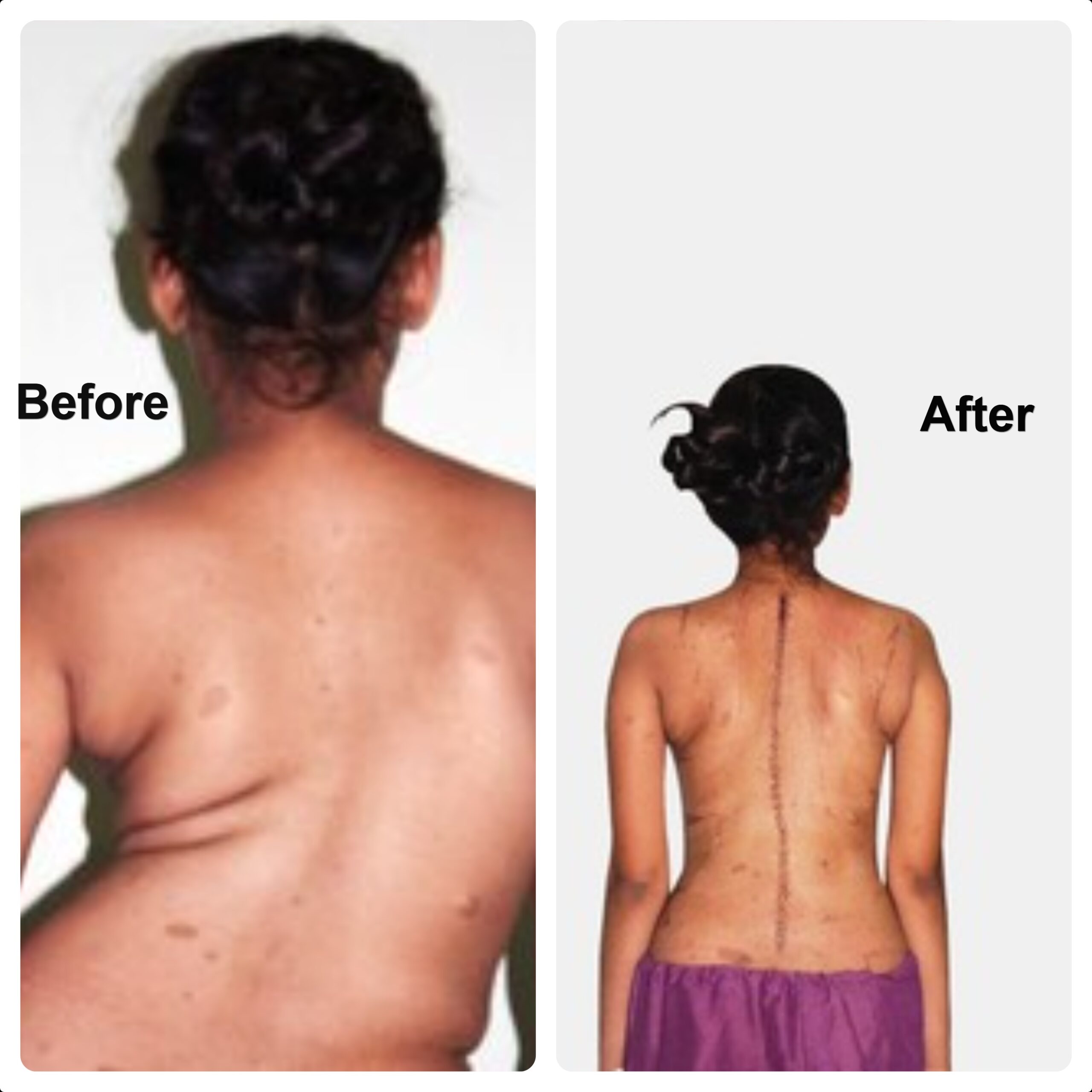
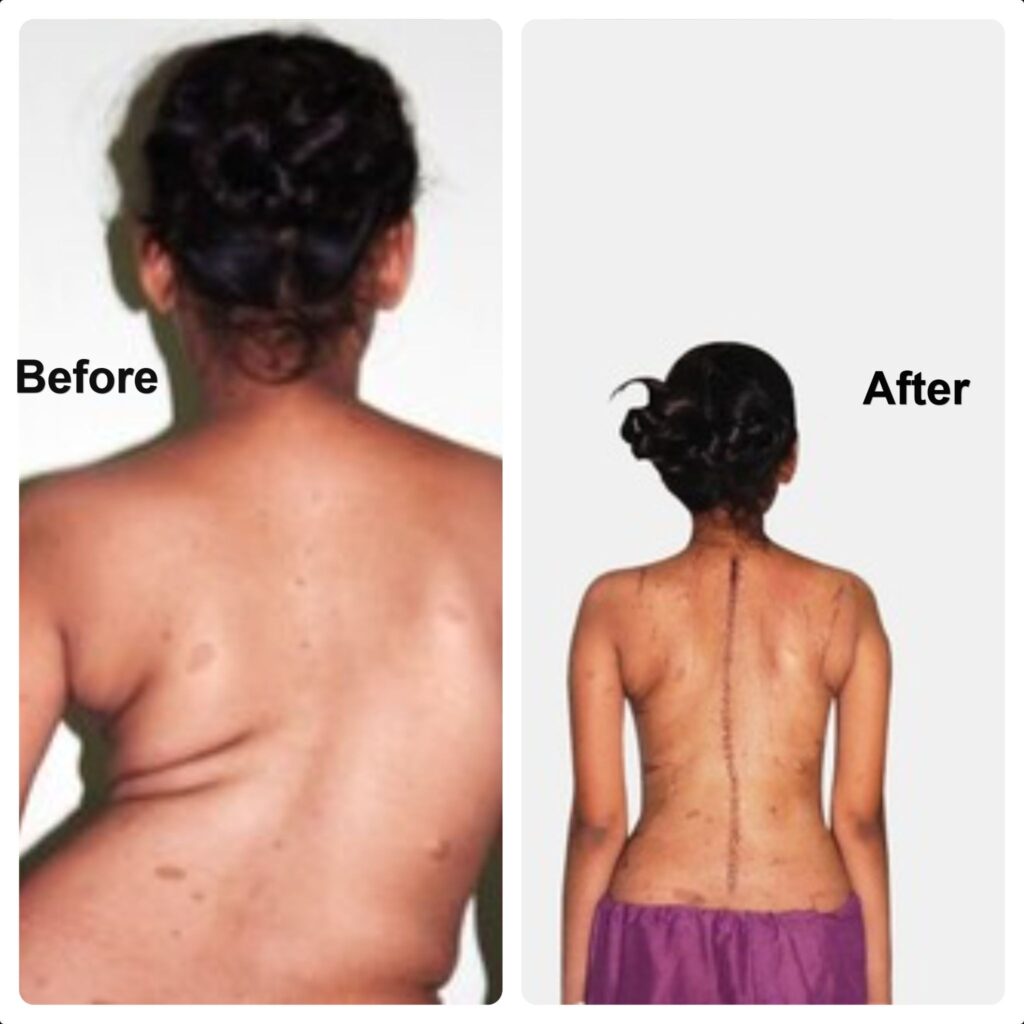
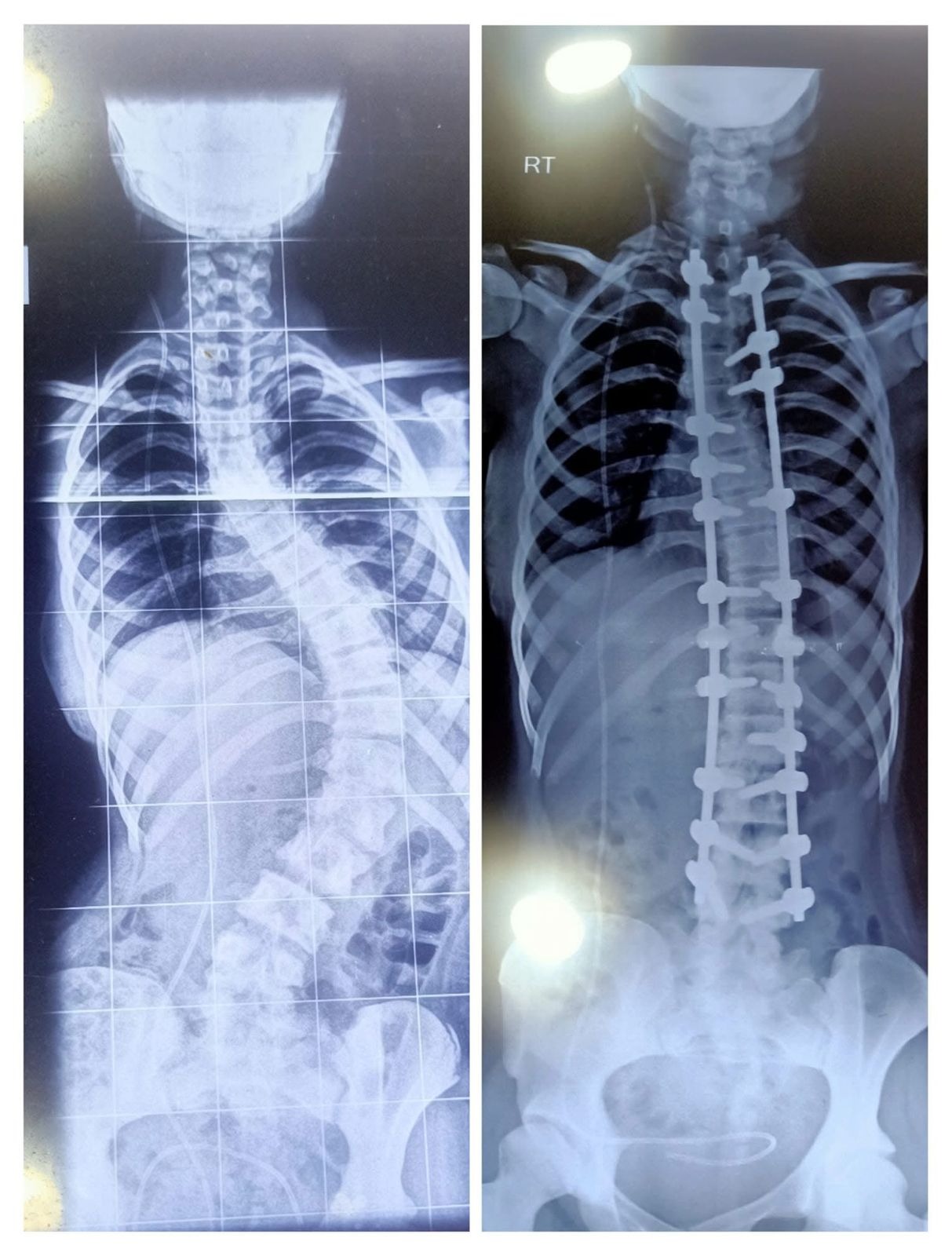
Realizing how much their daughter had suffered, her parents consulted a local orthopedic specialist, who referred them to Dr. B. Leela Prasad, a spine surgeon. After a detailed examination and standing X-rays, Chandana was diagnosed with adolescent idiopathic scoliosis, and her spinal curve measured nearly 70 degrees.
Dr. B. Leela Prasad explained that a curve of this magnitude was likely to progress further and recommended corrective spinal surgery. The word “surgery” terrified the family. They had expected medicines, exercises, or perhaps a brace—not a major spinal operation.
Fear Versus Hope
The family sought advice from relatives, friends, and neighbors. Almost everyone discouraged surgery.
“It is too risky.”
“What if she becomes paralyzed?”
“She’s only thirteen.”
“Let her live with the curve.”
Overwhelmed by fear, her parents decided against surgery.
When they told Chandana, she quietly asked, “So… I’m supposed to live like this forever?”
Her father tried to comfort her.
“A crooked back is better than risking your life.”
Chandana stood silently before the mirror. “You don’t understand.”
Every day people laugh at me. Every day I wish I didn’t have to step outside. I’m afraid of surgery. But I’m more afraid of living the rest of my life hiding from the world. Those words changed everything.
For the first time, her parents realized how deeply their daughter had suffered. While they focused on the operation’s risks, she endured a different, unseen pain. Over the next few days, they spoke again with Dr. B. Leela Prasad. He carefully explained the procedure, the expected benefits, the possible complications, and the precautions taken to make spinal deformity surgery as safe as possible. He answered every question patiently, ensuring that both Chandana and her parents understood the operation and what recovery would involve.
Gradually, fear gave way to informed confidence. This time, the decision was not driven by rumors or hearsay but by a clear understanding of the condition and the available treatment. With anxious hearts but renewed hope, Chandana’s parents gave their consent. They agreed to proceed with surgery.
Seven Hours That Changed Her Life
The day of the surgery finally arrived. On the morning of the operation, Chandana surprised everyone with her calmness. As she was wheeled toward the operating room, she gripped her mother’s hand tightly. “It’s going to be okay,” she whispered. Her parents watched the doors of the operating theater close behind her.
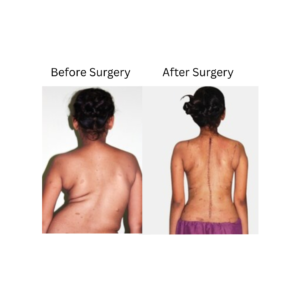
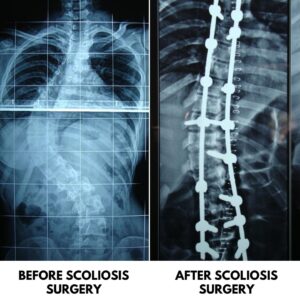
For them, the next seven hours felt endless. Inside the operating theater, the surgical team carefully exposed the curved portion of her spine. One by one, pedicle screws were inserted into the vertebrae along the planned levels. The screws were connected with strong titanium rods. Using modern spinal deformity correction techniques, the surgeons gradually restored her spine to a balanced alignment while continuously monitoring the spinal cord and nerves throughout the procedure. The prominent rib hump, produced by the rotation of the spine was also addressed by removing a small portion of the affected ribs, allowing the rib cage to assume a more symmetrical contour. The surgery had gone exactly as planned.
When Chandana woke up in the recovery room, she was in considerable pain, as expected after such a major operation. Even before she opened her eyes fully, she sensed something different. For months, whenever she lay on her bed, her body had rested unevenly because of the twisted curve in her spine. Now, for the first time in over a year, her back rested flat against the mattress. She smiled. Without looking into a mirror, she knew. Her back was straight.
Learning to Stand Tall Again
The days following surgery were challenging. Every movement caused discomfort. Sitting up required courage. Standing seemed almost impossible. Yet Chandana had already endured something far more painful than physical discomfort—the daily humiliation that had forced her to leave school and hide herself from the world. Compared with that emotional pain, the pain of recovery felt temporary.
Her resilience amazed everyone around her. On the second postoperative day, with the support of the physiotherapy team, Chandana stood upright for the first time after surgery. A few hesitant steps soon became a slow walk along the hospital corridor. Watching their daughter walk with a straighter posture brought tears of joy to her parents’ eyes.
Her recovery progressed remarkably well. The surgical wound healed uneventfully over the next two weeks, and each day she grew stronger, more confident, and more independent. Six weeks after surgery, Chandana returned to school. She wore the same uniform she had once been too afraid to put on. This time, she walked through the school gate with her shoulders relaxed and her head held high.
Some classmates were surprised to see her. Others came forward to welcome her back. The cruel whispers had disappeared. The mocking voices were silent. There were no more catcalls. For the first time in over a year, Chandana walked through the school corridors without fear. She laughed with her friends again. She answered questions in class. The girl who had once hidden herself from the world was slowly learning to stand tall—not just physically, but emotionally.
A New Beginning
Years passed. Chandana completed her education, married, and built the life she had once feared she would never have. Today, she is the proud mother of two daughters and works at Brandix, where her dedication and sincerity earn her respect. She is financially independent, a loving wife, and a caring mother.

Sometimes, while helping her daughters get ready for school, she remembers the morning when she herself refused to wear her school uniform. The memory no longer brings sadness. Instead, it fills her with gratitude—gratitude for her parents, who overcame their fears; gratitude for the doctors who treated her with skill and compassion; and gratitude for the opportunity to live the life she once thought she had lost.
More Than a Straight Spine
People often ask Chandana what changed her life. They expect her to talk about the operation. Instead, she smiles. “The surgery straightened my spine,” she says. “But courage straightened my life.”
Her parents, too, learned an unforgettable lesson. Fear had nearly prevented them from choosing the treatment their daughter needed. Looking back, they remain grateful that they ultimately placed their trust in expert medical advice rather than rumors and misconceptions.
The scar on Chandana’s back remains. She has never tried to hide it. To others, it is simply a surgical scar. To Chandana , it is a symbol of courage, resilience, and a second chance at life. Her journey is not merely about scoliosis surgery.
It is about a young girl whose dreams were interrupted by a spinal deformity, whose confidence was shattered by cruelty, and whose future was restored through timely diagnosis, compassionate medical care, unwavering family support, and extraordinary determination.
Today, when people meet Chandana, they do not see scoliosis. They see a confident woman. A devoted wife. A caring mother. Few realize that years earlier, this same girl had been too frightened to walk out of her own front door.
This is the story of Chandana—a young girl who refused to let a curve define her future and chose to stand tall for the rest of her life.







 Key Message:
Key Message:
 Myth 1: “Carrying heavy school bags/backpacks causes scoliosis.”
Myth 1: “Carrying heavy school bags/backpacks causes scoliosis.”