Common Myths About Spine Surgery
1. Myth: Spine surgery is always the first treatment for back pain
Fact:
Most spine problems do not require surgery. The majority of patients improve with a short period of rest, appropriate medications, physiotherapy, and lifestyle changes.
Surgery is considered only in a small percentage of cases—typically when these treatments do not provide relief or when there is significant nerve compression causing severe symptoms.
2. Myth: Spine surgery is only for elderly patients.
Fact:
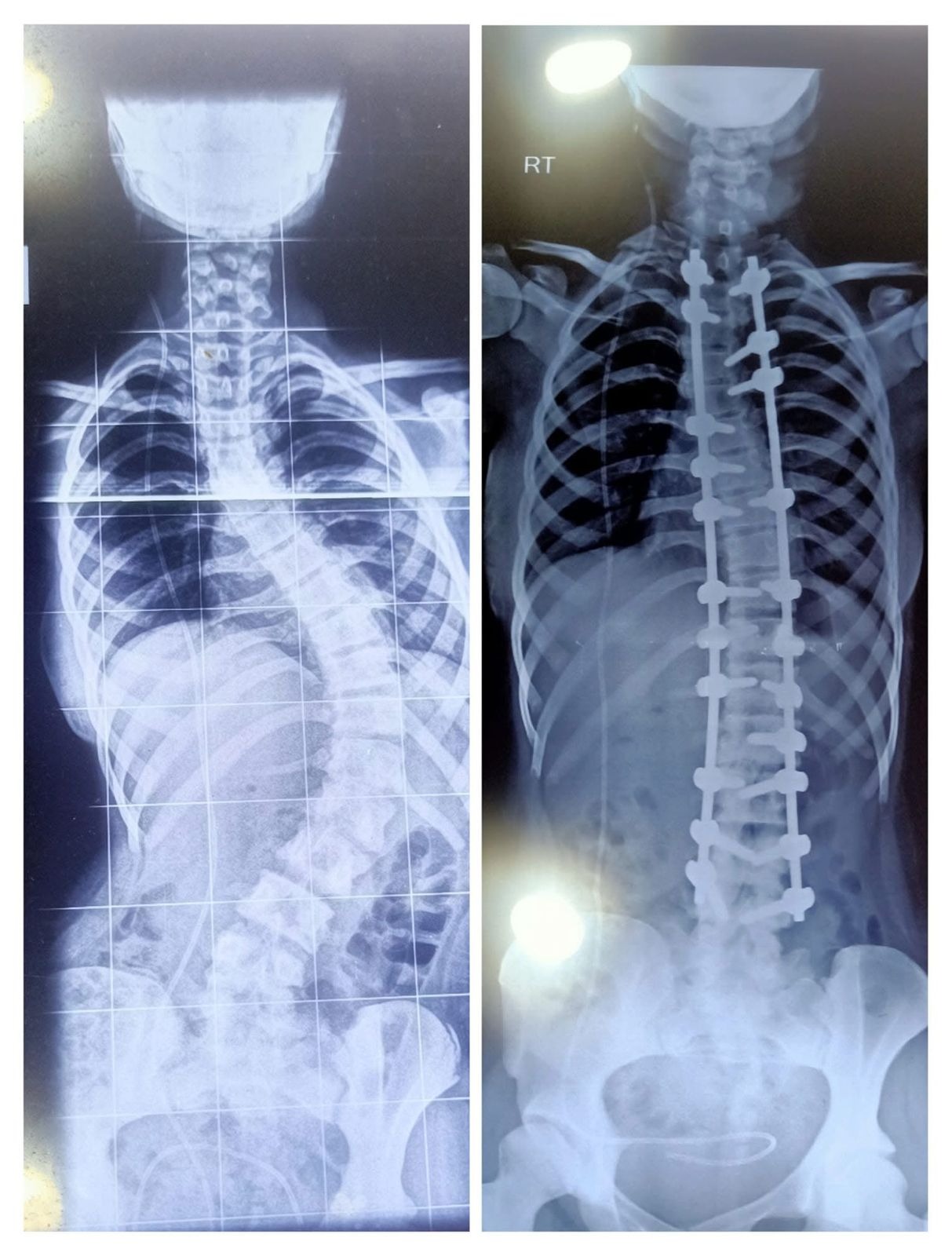
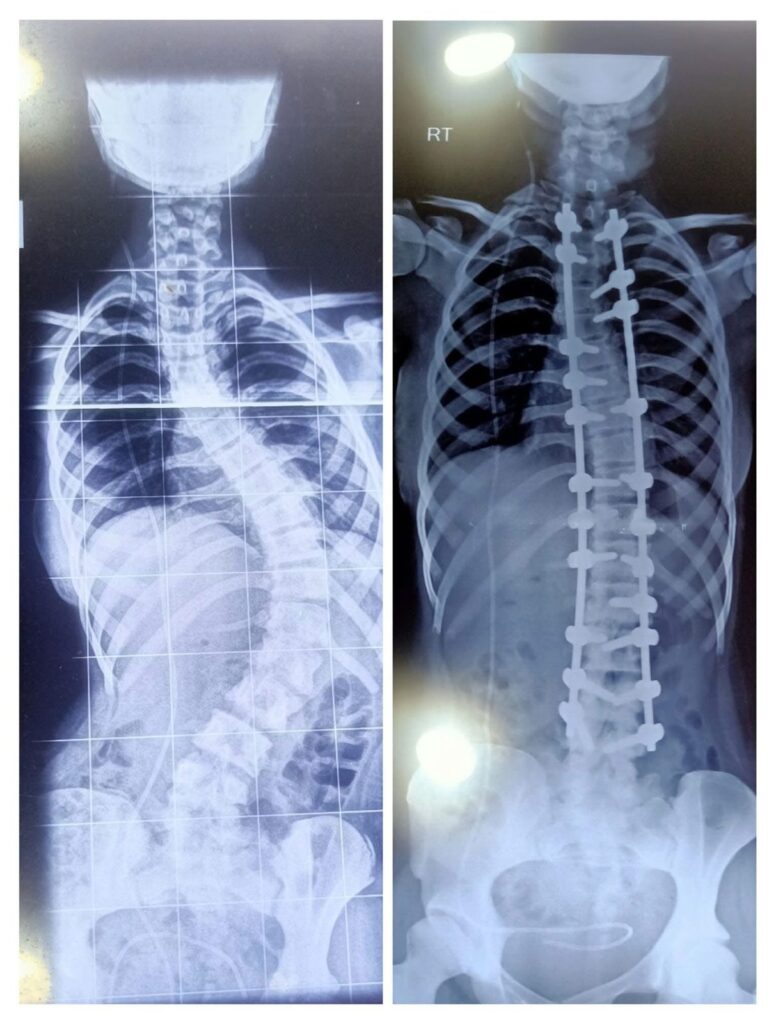
Spine surgery may be required in people of any age, depending on the condition. Problems such as disc prolapse, spondylolisthesis, fractures, deformities, infections, or tumors can occur in younger as well as older individuals.
3. Myth: Spine surgery, when required, must always be done as an emergency or else the patient will become paralyzed
Fact:
Most spine surgeries are not emergencies and can be safely planned after proper evaluation and imaging.
Emergency surgery is needed only in specific situations, such as:
- Severe spinal cord compression causing rapidly progressing weakness of limbs and/or loss of bowel and bladder control
- Spinal trauma causing instability
A spine specialist will determine whether surgery is urgent, elective, or not required, based on the patient’s condition.
4. Myth: Spine surgeons recommend surgery for all patients.
Fact:
This is a common misunderstanding. Spine surgeons treat the majority of patients without surgery using medications, physiotherapy, exercise, and lifestyle changes. Spine surgeons are specially trained to diagnose spine problems and decide the most appropriate treatment, whether non-surgical or surgical. Surgery is recommended only when necessary.
5. Myth: Spine surgery is always very risky.
Fact:
Modern spine surgery has become much safer due to advances in surgical techniques, better imaging, improved anesthesia, and enhanced perioperative care. Many procedures today are minimally invasive, which means smaller incisions, less tissue damage, and faster recovery.
Patients are carefully evaluated before surgery, and the benefits, risks, and alternatives are thoroughly discussed.
6. Myth: Spine surgery leaves large scars and requires long hospital stays.
Fact:
Many spine surgeries today are minimally invasive, involving smaller incisions, less muscle damage, shorter hospital stays, and faster recovery.
7 Myth: Spine surgery requires months of bed rest.
Fact:
With modern techniques, patients are usually encouraged to start walking within a day or two after surgery. Early mobilization helps recovery and reduces complications.
8. Myth: Recovery after spine surgery is very slow.
Fact:
Recovery after spine surgery varies depending on the severity and duration of the underlying condition, the type of surgery performed, and the patient’s overall health. With proper rehabilitation and medical guidance, many patients are able to return to their daily activities within a few weeks.
However, in certain situations—especially when the spinal cord or nerves have been compressed for a long time before surgery—recovery may take longer. In such cases, improvement is often gradual and may sometimes be incomplete, depending on the extent of nerve damage prior to treatment.
9. Myth: Patients cannot return to sports or dancing after spine surgery.
Fact:
After proper recovery and rehabilitation, many patients can return to sports, exercise, and dancing, depending on the type of surgery and medical advice.
10. Myth: Spine surgery means permanent disability.
Fact:
Most patients return to normal daily activities, work, and exercise after recovery.
11. Myth: The risk of nerve injury or paralysis after spine surgery is very high.
Fact:
The risk of nerve injury or paralysis is very low in most spine surgeries. Even in complex procedures, the risk is generally low when surgery is performed by experienced spine surgeons using modern techniques and safety measures.
Many spine operations are actually performed to relieve pressure on nerves or the spinal cord and prevent permanent nerve damage.
12. Myth: Once you have spine surgery, you will need repeated surgeries.
Fact:
Most patients do not require repeat surgeries. When surgery is performed for the right indication and followed by proper rehabilitation, many patients experience long-term relief.
However, some spine conditions, such as disc prolapse, can recur over time, and natural aging may lead to degeneration at other levels of the spine. Hence, a small percentage of patients may require additional surgery later.
13. Myth: Eating dal after spine surgery causes surgical wound infection.
Fact:
Eating dal does not cause wound infection. In fact, dal is a rich source of protein, which is essential for wound healing and recovery after surgery.
Wound infections (surgical site infections) are usually caused by germs entering the surgical wound during or after surgery. Several factors can contribute to this, including a breach in sterile technique, inadequate sterilization of instruments or the operating environment, excessive tissue handling, or blood loss during surgery.
Patient-related factors such as uncontrolled diabetes, obesity, poor hygiene, low immunity, smoking, and improper wound care after surgery also increase the risk.
14. Myth: Spine surgery should be done only by neurosurgeons.
Fact:
Spine surgery is performed by both neurosurgeons and orthopedic spine surgeons who have specialized training in spine care.
- Neurosurgeons traditionally focus more on intradural problems such as spinal cord tumors and nerve-related conditions.
- Orthopedic spine surgeons often focus more on extradural problems such as spinal malalignment, deformities, fractures, and spinal stabilization.
The most important factor is the surgeon’s expertise, training, and experience in spine surgery.
15. Myth: Major spine surgeries are done only in metro cities.
Fact:
Major spine surgeries are no more limited to metro cities. With advancements in medical technology and training, many well-equipped hospitals in smaller cities and towns are now capable of performing complex spine procedures safely and effectively.
Qualified spine surgeons, modern operation theatres, advanced imaging, and improved anesthesia care are increasingly available beyond metro areas. As a result, patients can often receive high-quality spine care closer to home.
16. Myth: It is better to avoid spine surgery at all costs.
Fact:
When surgery is recommended for the right reasons and at the right time, it can relieve severe pain, protect nerves, and significantly improve quality of life.
✅ Key Message:
Spine surgery is not required for most patients, but when necessary, it can be safe, effective, and life-changing, helping relieve pain and restore normal function.
Best Spine Surgeon in Vizag – Dr. B. Leela Prasad, Amulya Hospital
Dr. B. Leela Prasad is one of the most trusted and experienced spine surgeons in Vizag, currently practicing at Amulya Hospital. With many years of experience in orthopaedics and spine surgery, he specializes in treating conditions such as slip disc, sciatica, spinal deformities, and complex spine infections.
Known for his patient-centric approach, Dr. Leela Prasad focuses on accurate diagnosis and prefers non-surgical treatments whenever possible, recommending surgery only when necessary. He is skilled in advanced and minimally invasive spine procedures, ensuring faster recovery and better outcomes for patients.
At Amulya Hospital, patients benefit from modern facilities, advanced technology, and personalized care, making it a reliable destination for comprehensive spine treatment in Visakhapatnam.
Dr. B Leela Prasad