Dr. B. LEELA PRASAD
SPINE SURGEON
AMULYA HOSPITAL
Common Myths About Scoliosis
Myth 1: “Carrying heavy school bags/backpacks causes scoliosis.”
Truth: Carrying heavy school bags may cause temporary back or shoulder pain, but it does not cause scoliosis.
A heavy bag can strain muscles, but it will not permanently change the shape of the spine.
Myth 2: “Scoliosis is caused by poor posture.”
Truth: Poor posture does not cause scoliosis. Slouching may make asymmetry more noticeable, but it does not create a structural spinal curve.
Myth 3: “Scoliosis only affects girls.”
Truth: Both boys and girls can develop scoliosis. However, girls are more likely to have curves that progress and require treatment.
Myth 4: “Scoliosis always causes visible deformity.”
Truth: Many scoliosis curves are mild and barely noticeable. Possible signs include uneven shoulders, rib prominence, or waist asymmetry — but not everyone has obvious physical changes.
Myth 5: “Scoliosis is painful.”
Truth: Scoliosis in children and adolescents is usually painless. Pain is more common in adults with long-standing curves or degenerative changes, but many people with scoliosis live completely pain-free.
Myth 6: “Scoliosis can be corrected by exercise and physiotherapy.”
Truth: Exercise and physiotherapy improve strength, posture, and comfort — but they usually do not permanently straighten a structural curve.
Specialized programs such as the Schroth method may help manage progression and improve symmetry, but they are not a guaranteed cure.
Myth 7: “Braces cure scoliosis.”
Truth: Bracing does not cure scoliosis. It helps prevent the curve from worsening while a child is still growing.
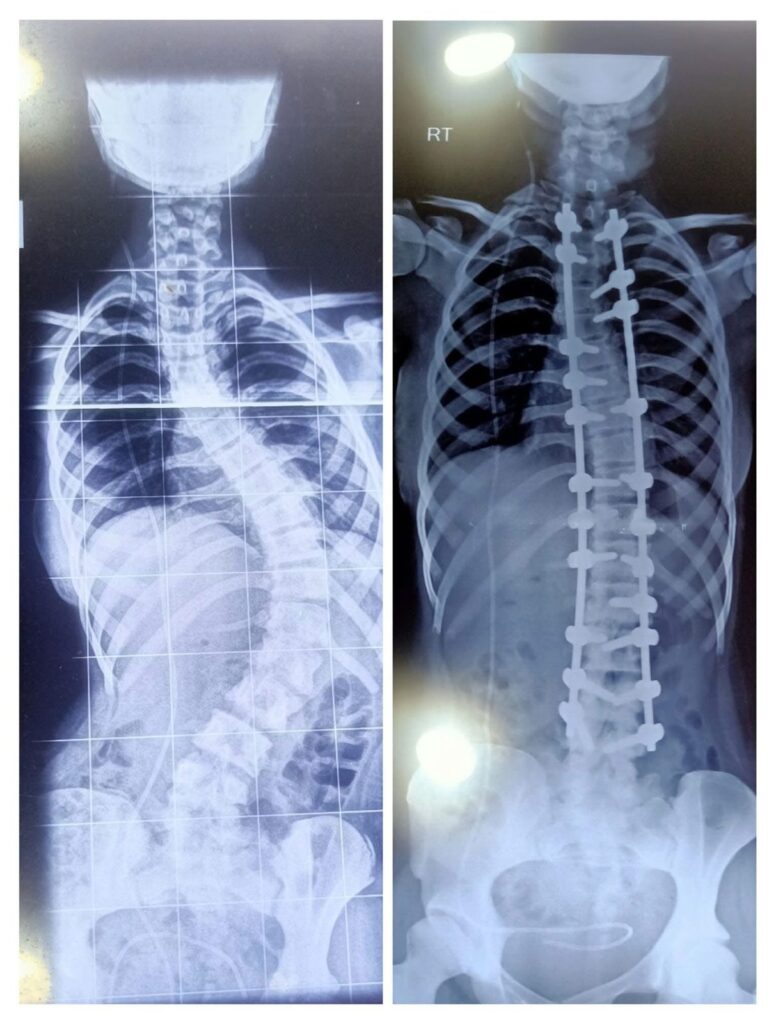
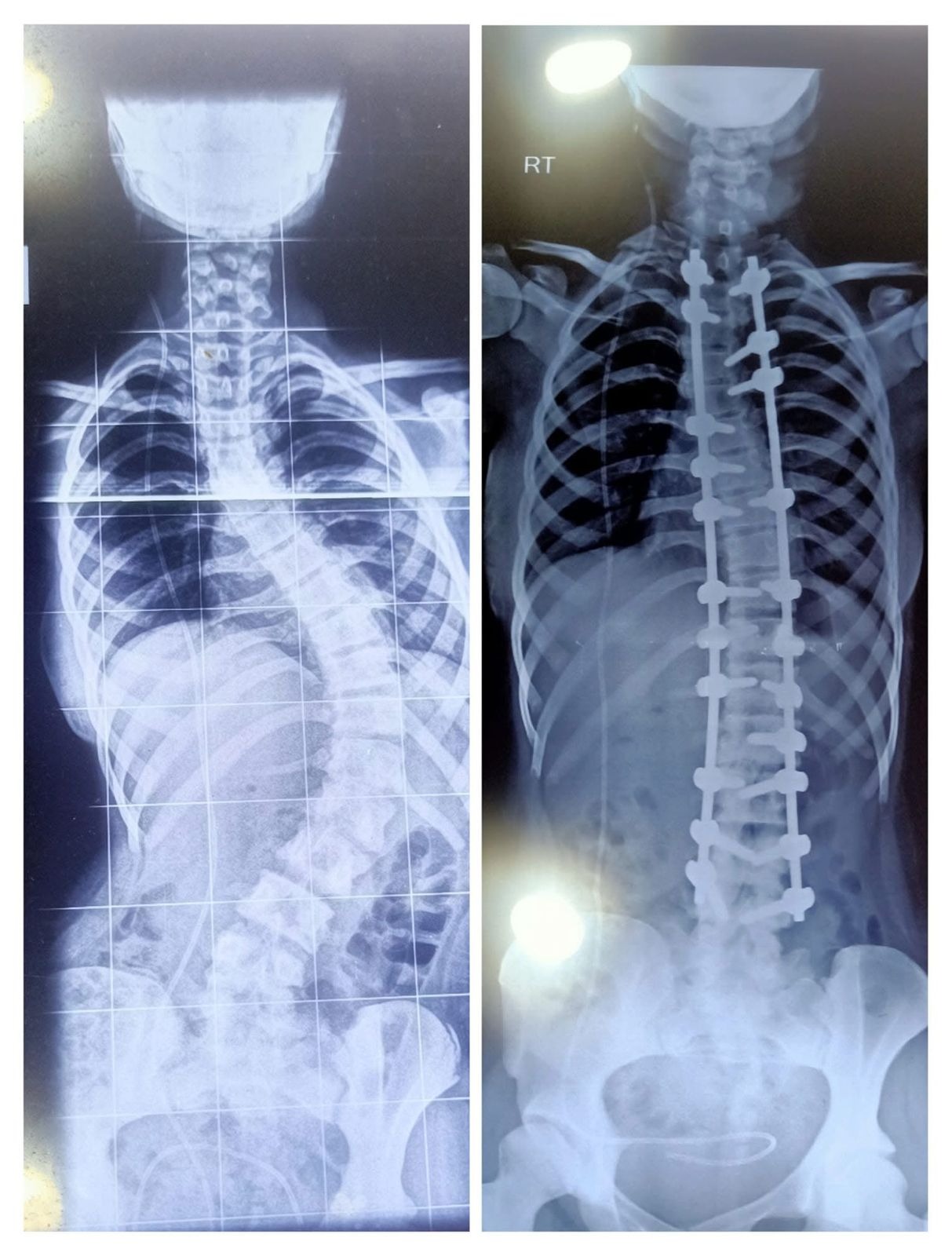
Myth 8: “Everyone with scoliosis needs surgery.”
Truth: Surgery is recommended only for severe or rapidly progressing curves. Most patients are either monitored regularly or treated with bracing.
Myth 9: “If you need surgery, you’ll never be active again.”
Truth: Most patients return to sports, dance, and everyday activities within a few months after surgery.
Although procedures like Spinal fusion may reduce flexibility in the treated segments, patients are generally encouraged to remain active once healing is complete.
Myth 10: “Females cannot have normal childbirth after scoliosis surgery.”
Truth: Most women who undergo scoliosis correction surgery can conceive normally, carry pregnancy safely, and deliver vaginally.
Scoliosis surgery does not affect the uterus, ovaries, or hormonal function, so fertility is typically unaffected.
Myth 11: “Children stop growing taller after scoliosis correction surgery.”
Truth: Children do not automatically stop growing after scoliosis surgery.
Most procedures are performed near or after the adolescent growth spurt, when most spinal growth is already complete.
Many children actually become taller immediately after surgery because the curved spine is straightened.
Spinal fusion stops growth only in the fused segments. Growth of the unfused spine, legs, and the rest of the body continues until skeletal maturity.
In very young children with early-onset scoliosis, surgeons may use growth-friendly techniques instead of full fusion to allow continued spinal growth.
Myth 12: “Scoliosis surgery is very risky and often causes serious complications like paralysis.”
Truth: Scoliosis correction is a complex procedure, but with modern techniques and intraoperative monitoring, it is considered safe when performed by experienced spine deformity surgeons.
Serious complications such as paralysis are very rare.
Myth 13: “Complex spine surgeries can only be done in major metropolitan cities.”
Truth: In the past, scoliosis correction was largely concentrated in metropolitan centers due to the need for highly specialized surgeons, advanced ICUs, experienced anesthesia teams, and specialized instrumentation.
Over the past 10–15 years, spine care has advanced significantly. Surgical expertise, modern technology, and advanced hospital infrastructure are now available in many Tier 2 cities.
As a result, complex spine surgeries such as scoliosis correction can be safely and successfully performed in well-equipped centers—including cities like Visakhapatnam—provided the necessary expertise, technology, and multidisciplinary support are in place.
For scoliosis treatment in Visakhapatnam, one needs to consult a top spine surgeon in Visakhapatnam. Visit Dr. B. Leela Prasad, one of the best scoliosis consultation specialists in Vizag. These are some common myths about scoliosis that people believe.